Understand fetal physiology, the changes that occur at birth, and resultant neonatal physiology
Identify the parts of the developing heart tube
Know the heart tube precursors and their cardiac derivatives
Be able to explain how atrial, ventricular, and truncal septation occurs
Understand normal arch development and common arch variants
Understand development of systemic venous return and common variants
Understand basic cardiac defects and their physiologic implications
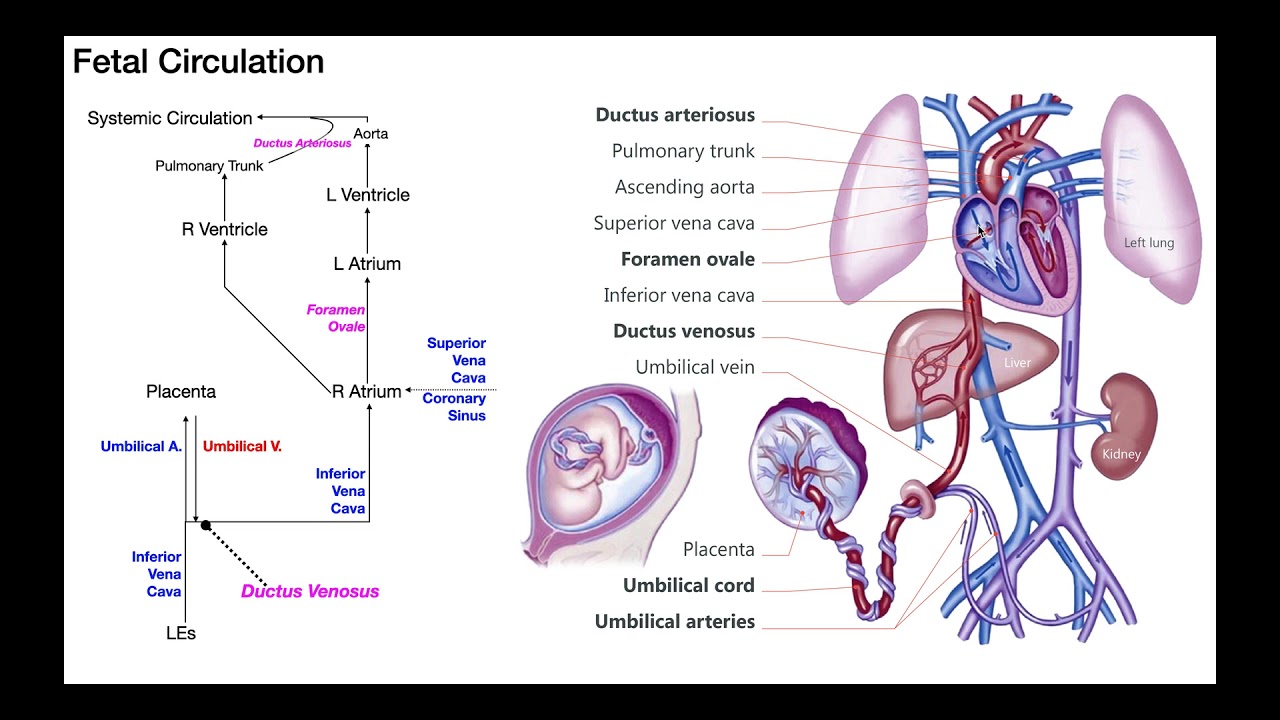
Fetal Circulation
Fetal Circulation Pathway
Oxygenated blood from the mother enters the fetus through the umbilical vein.
It traverses the liver through the ductus venosus to enter the inferior vena cava (IVC) and then into the Right Atrium.
The majority of this blood then streams across the Foramen Ovale into the Left Atrium, Left Ventricle, Ascending Aorta to head, neck, arms, and some to the body.
Superior vena cava (SVC) returns to the Right Atrium and primarily crosses the Tricuspid Valve into the Right Ventricle and out the Pulmonary Artery. Due to high pulmonary vascular resistance in utero, very little blood flow enters the branch of the pulmonary artery. Most blood entering the pulmonary artery is shunted through the ductus arteriosus and down the descending aorta to the low-resistance placental bed.
At Birth
The umbilical cord is clamped, removing the low resistance placenta.
Systemic Vascular Resistance rises.
As the baby begins to breathe, the oxygen content of the blood increases.
Pulmonary Vascular Resistance begins to fall and more blood flows into the lungs.
With increased blood oxygen, the Ductus Arteriosus constricts (1-2 days to close).
Increased pulmonary venous return to the Left Atrium raises left atrial pressure, reversing the shunt through the Foramen Ovale.
Over time, the flap valve of the Foramen Ovale is pushed against the septum and usually seals the atrial septum (a few weeks to months).
Early Vascular Systems
Formation of Blood Vessels
At approximately 20 days, multiple blood islands form in the cephalic portion of the embryonic cardiogenic plate.
These blood islands coalesce to form primitive vascular channels, which fuse and form a pair of heart tubes.
By day 22-23, the heart begins to beat, initially resembling a peristaltic wave more than a true heartbeat.
Heart Tube Formation
Lateral infolding brings the two heart tubes into apposition, and they fuse around day 22 to form the primitive heart tube.
The heart tube grows rapidly within the pericardial cavity, undergoing twisting or 'looping,' which typically results in a rightward twist, creating an anterior-posterior structure.
Chambers of the Heart Tube
Around day 23: The heart's regions are identifiable as truncus arteriosus, bulbus cordis, ventricle, atrium, and sinus venosus.
The heart grows rapidly within the pericardial cavity, and looping twists the tube into its final orientation.
By the end of week 4, the venous pole and atria lie posterior and superior to the primitive ventricle, bulbus cordis, and truncus arteriosus.
Atrial Septation
Atrial Septal Development
Tissue from the roof of the primitive atrium grows down toward the endocardial cushions, forming septum primum, with foramen primum as the initial opening.
Septum primum continues to grow and fuse with the endocardial cushions, but fenestrations begin forming within it, creating foramen secundum as they coalesce.
Septum Secundum and Foramen Ovale
Septum secundum begins to grow from the top of the atrium on the right atrial side of septum primum, creating an inverted 'C' shape and leaving a gap known as the foramen ovale.
Post-birth, rising left atrial pressure pushes the septum primum flap against the septum secundum, eventually leading to the closure of foramen ovale.
Ventricular Septation
Septation of the Ventricles and Truncus Arteriosus
During week 4, the interventricular septum begins forming within the trabeculated portion of the ventricle.
Truncal septation starts in week 5, involving neural crest cells migrating into the outflow tracts.
Bulbar ridges form and fuse to divide the truncus arteriosus into the aorta and pulmonary artery, completing the septation process.
Arch Development
Aortic Arch Development
The 6 pairs of embryonic arches connect the trunco-aortic sac to the dorsal aorta.
The 3rd set forms the common and internal carotid arteries.
Right 4th arch regresses, with remnants at the junction of the right common carotid artery and right subclavian artery, while the left 4th arch persists as part of the aortic arch.
6th arch contributes to the pulmonary arteries and ductus arteriosus.
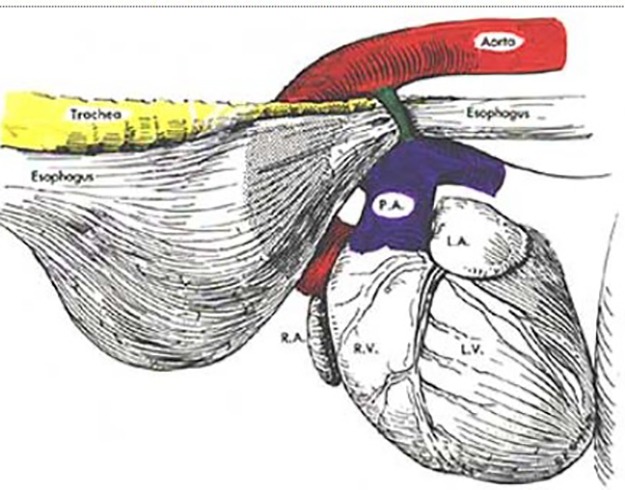
Arch Anomalies
Abnormal arch development can lead to conditions such as vascular rings, which can compress the trachea and esophagus, causing respiratory or digestive issues.
A double aortic arch or a right aortic arch with a left-sided diverticulum of Kommerell can form vascular rings requiring intervention.
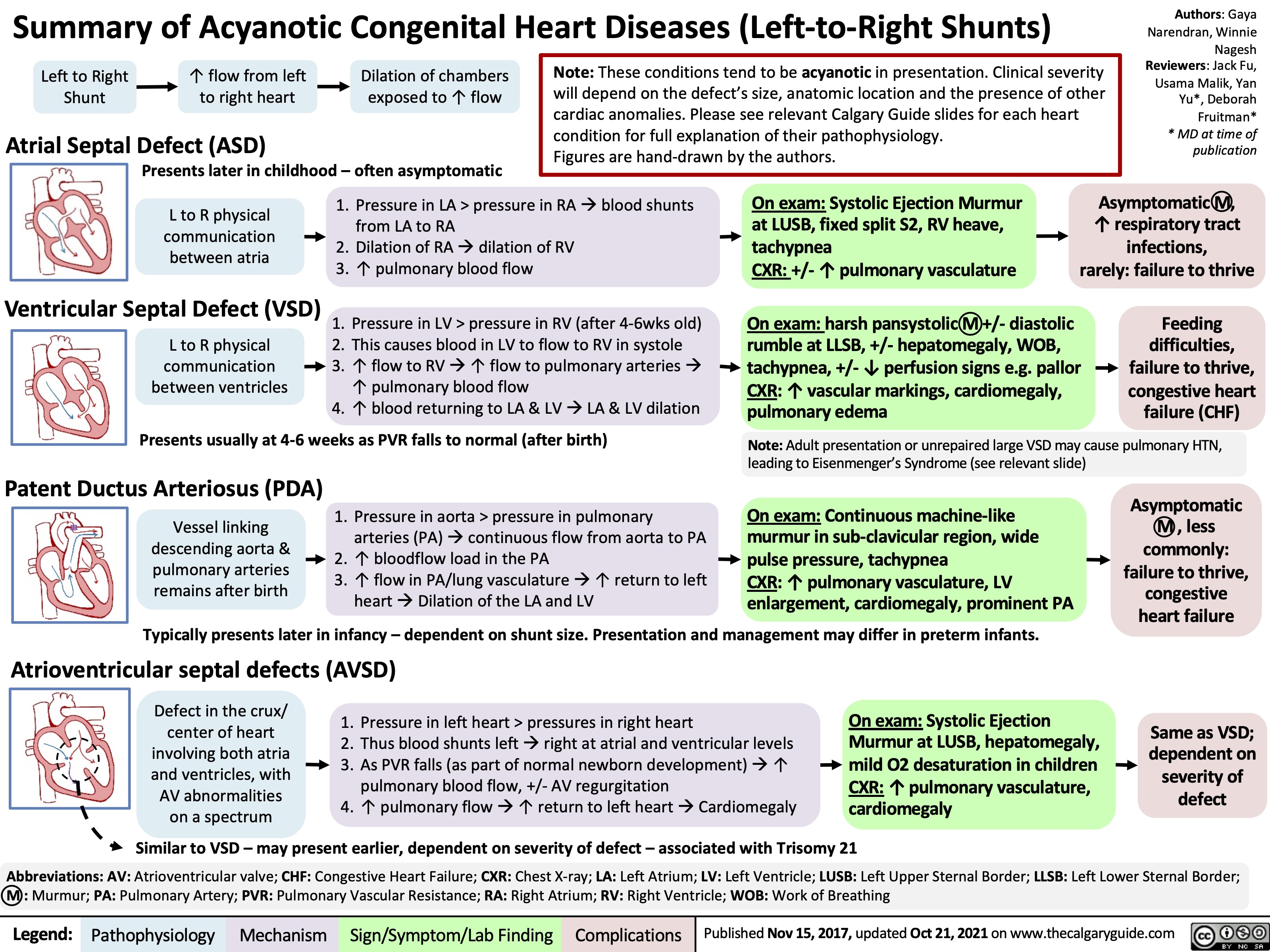
Congenital Heart Defects
Patent Ductus Arteriosus (PDA)
Failure of the ductus arteriosus to close results in a left-to-right shunt and more frequent in premature infants.
Can lead to Eisenmenger syndrome and differential cyanosis (pink fingers, blue toes).
Atrial Septal Defects (ASDs)
Include secundum, primum, and sinus venosus types.
Cause left-to-right shunting and right heart dilation.
Ventricular Septal Defects (VSDs)
Most common congenital heart_defects, named by their position