ECG in Ischemia and Acute Myocardial Infarction
ECG in Ischemia and Acute Myocardial Infarction

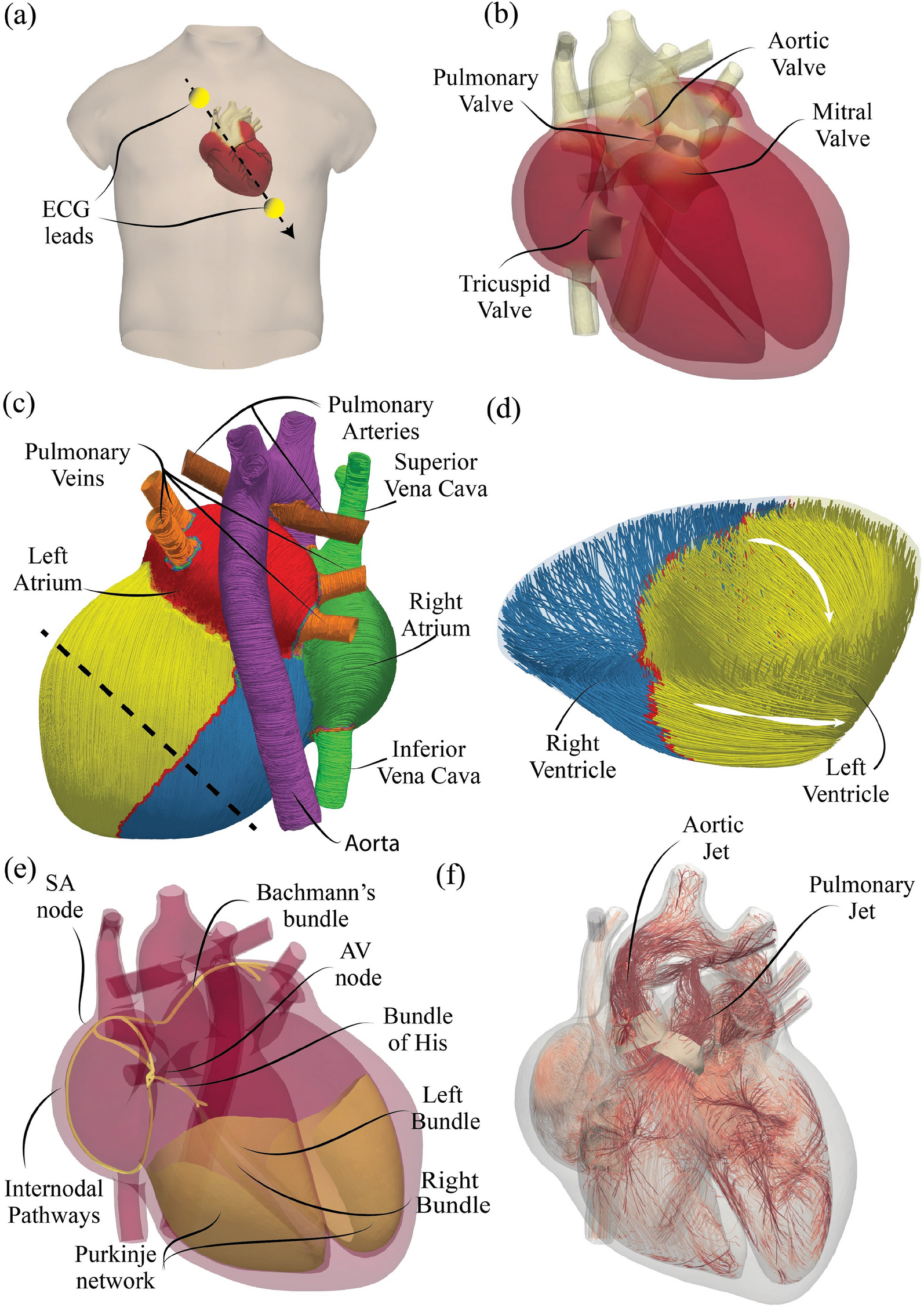
Anatomy Review
To understand the ECG changes in ischemia and acute myocardial infarction (AMI), it is essential to review the anatomy of the coronary arteries and their corresponding ECG leads.
Coronary Arteries
- Left Main Coronary Artery: Splits into the Left Anterior Descending (LAD) artery and Circumflex artery.
- Circumflex Artery: Supplies the lateral wall of the left ventricle.
- Right Coronary Artery (RCA): Supplies the right atrium, right ventricle, and part of the left ventricle.
- Left Anterior Descending (LAD): Supplies the anterior wall and septum of the left ventricle.
- Branches: Includes septal, obtuse marginal, diagonal, right posterolateral, and posterior descending artery.
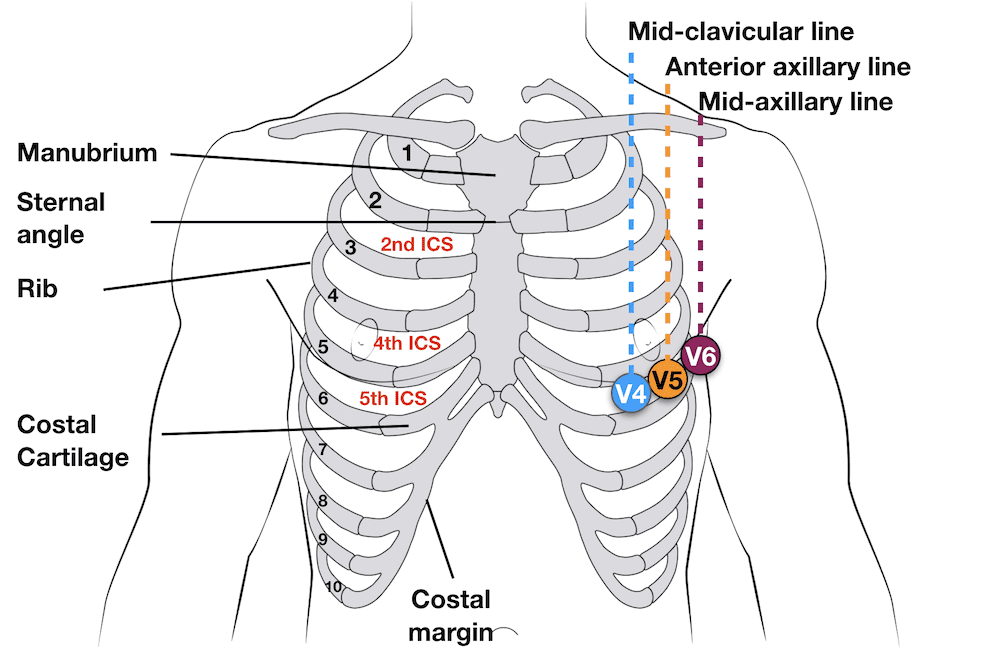
Leads and Cardiac Anatomy
ECG Leads: Different ECG leads provide information about different areas of the heart:
- Inferior Leads (II, III, aVF): Reflect the inferior part of the heart, mainly supplied by the RCA or Circumflex artery.
- Lateral Leads (I, aVL, V5, V6): Reflect the lateral wall of the heart, mainly supplied by the Circumflex artery.
- Anterior Leads (V3, V4): Reflect the anterior wall of the heart, mainly supplied by the LAD.
- Septal Leads (V1, V2): Reflect the septum, mainly supplied by the LAD.
- Intermediate Leads (aVR, aVL): Provide additional views.
Anatomy on ECG
- Lateral Leads: aVR, aVL, V2, V4, V5, V6
- Inferior Leads: aVF, V3
- Anterior-Septal Leads: V1, V2, V3, V4
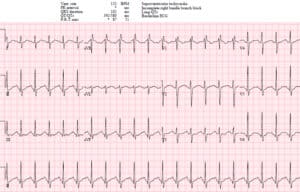
Case Discussions and ECG Interpretation
Case 1: 60-Year-Old Man with Severe Mid-Chest Discomfort
Symptoms: Severe oppressive discomfort in the mid-chest and upper abdomen that began four hours ago.
ECG Findings: - ST Elevation: Inferior-Lateral Leads (II, III, aVF) - Interpretation: Acute Inferior-Lateral Myocardial Infarction involving RCA or LCX as the culprit vessel.
Case 2: 41-Year-Old Man in Coronary Care Unit
Symptoms: Severe chest pain.
ECG Findings: - ST Elevation: Anterior-Septal-Lateral Leads (V1/V2/V3/V4, V5/V6, I, aVL) - ST Depression: Inferior Leads - Interpretation: Acute Anterior-Septal-Lateral Myocardial Infarction involving the proximal LAD as the culprit vessel.
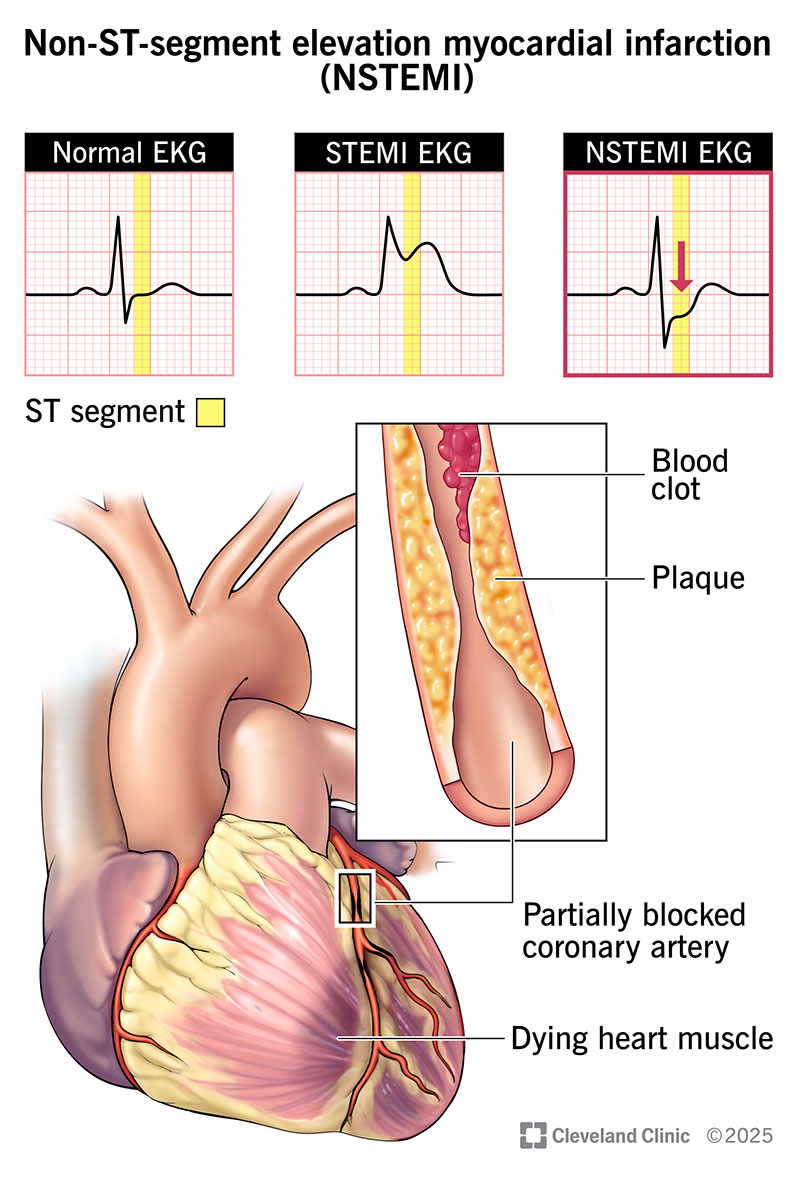
ST-Segment and Myocardial Injury
Understanding ST-Segment: - ST Elevation: Represents injury, usually epicardial or transmural. Criteria: >1 mm in >2 leads, indicates ST Elevation MI (STEMI). - ST Depression: Represents ischemia, indicates injury to the endocardium. Criteria: >1 mm in >2 leads, indicates Non-ST Elevation MI (NON-STEMI).
Causes of ST Elevation
- Current of Injury Concept: The true cause is unknown and controversial, but the current of injury is a simpler way to understand it.

Common Clinical Cases and Management
Unstable Patient with Wide QRS Complex
Symptoms: Hemodynamically unstable patient presents with a supraventricular tachycardia with a wide QRS complex.
Management: Emergent cardioversion should be considered.
Case Studies for Practice
- ST Elevation in Lead I: Indicates an inferior-lateral MI.
- Atrial Fibrillation: Identified by irregular rhythm.
- Ventricular Tachycardia: Wide QRS complex, requires immediate intervention.
Post-MI Management
After a successful stenting of the RCA or other interventions: - Monitor for Ventricular Arrhythmias: Short runs of ventricular tachycardia commonly occur post-MI. - Medications: Lidocaine is often used in the treatment of ventricular tachyarrhythmias post-MI.
Case 3: 70-Year-Old Man with Diabetes and Substernal Chest Pain
Symptoms: Substernal chest pain, appears in distress.
ECG Findings:
- Diagnosis: ST elevation myocardial infarction
- Pathophysiology: Thrombus occluding a coronary artery
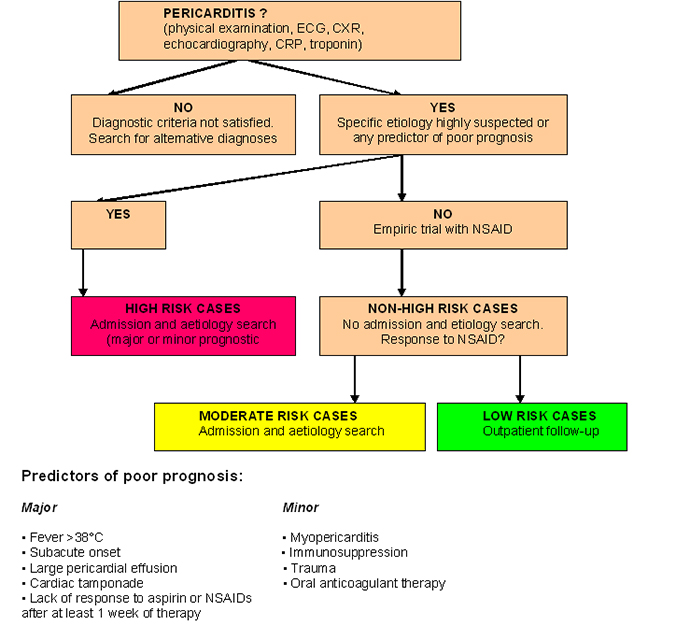
Treatment of Acute Pericarditis
Symptoms: Chest pain that increases with inspiration and is better with sitting up.
Etiology: Inflammatory, infectious, post-MI, medication-induced, tumor, trauma.
Treatment: Anti-inflammatory agents (high dose aspirin, NSAIDs, colchicine, rarely steroids).