Approach to Reading a 12-Lead ECG
Approach to Reading a 12-Lead ECG
Reading a 12-lead electrocardiogram (ECG) involves a systematic approach. Below are the key components:

Method for Reading an ECG
- Rate
- Rhythm
- Axis
- Measurements
- P-Waves
- PR Interval
- QRS Complex
- ST Segment
- T-Waves
- QT Interval
P-Waves
- Atrial Depolarization
- Normal Parameters:
- 2-3 small boxes wide
- < 2 small boxes tall
- Positive in inferior leads and biphasic in V1
P Wave Abnormalities
- Abnormal P wave morphology
- Different P wave morphologies
- Absent P waves (Atrial conduction abnormalities)
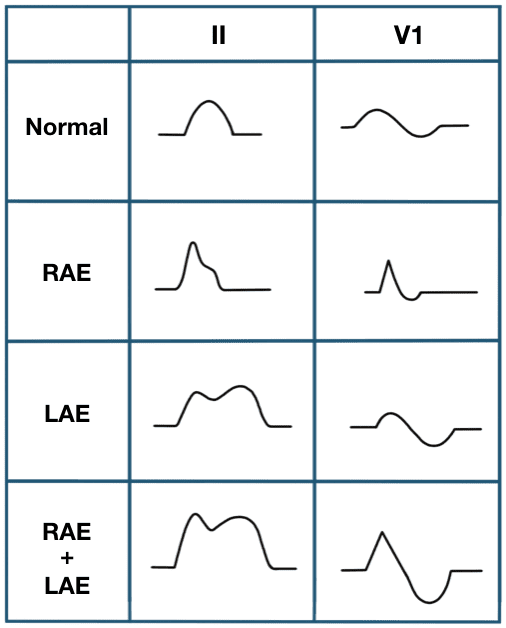
Atrial Conduction Abnormalities
- Right Atrial Abnormality (RAA)
- Left Atrial Abnormality (LAA)

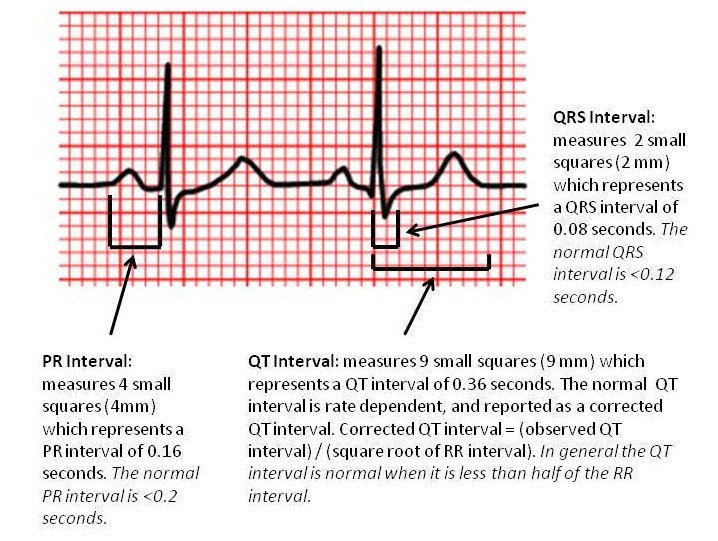
PR Interval
- Normal: Between 0.12 (3 small boxes) & 0.20 seconds (5 small boxes)
- Measured From: Beginning of P-wave to beginning of QRS complex
- Function: AV Nodal Conduction/Slowing
- Abnormalities:
- Too Long (>0.20 sec): AV-nodal/His-Purkinje system block (e.g., 1st, 2nd, or 3rd-degree block)
- Too Short (<0.12 sec): Accessory Pathway (e.g., Wolff-Parkinson-White (WPW) Syndrome)
AV Nodal Block
- 1st Degree AV Block: Atrioventricular conduction lengthened (P-wave precedes each QRS-complex but interval is > 0.2 s)
- 2nd Degree AV Block (Mobitz Type I): Intermittent non-conducted P waves without PR prolongation
- 2nd Degree AV Block (Mobitz Type II): P-waves look similar; successively longer PRIs until one QRS fails
- 3rd Degree AV Block: Complete absence of AV conduction, ventricular contraction occurs either due to a junctional or ventricular pacemaker

Wolff-Parkinson-White (WPW) Syndrome
- Short PR-Interval (<0.12sec) & Widened QRS Complex
- Delta Wave: Pre-excitation through Accessory Pathway
- Risks: Tachyarrhythmias, Re-entrant tachycardia, Atrial fibrillation/flutter, Ventricular tachycardia/fibrillation
QRS Complex
- Ventricular Depolarization
- Normal: <0.12 sec (3 small boxes)
