Renin-Angiotensin-Aldosterone System Inhibitors
Renin-Angiotensin-Aldosterone System Inhibitors (RAAS Inhibitors)

What Are Renin-Angiotensin-Aldosterone System Inhibitors?
Drugs that inhibit distinct portions of the renin-angiotensin-aldosterone system (RAAS) include angiotensin-converting enzyme (ACE) inhibitors, angiotensin-receptor blockers (ARBs), and renin inhibitors. The RAAS comprises hormones that regulate the body's blood pressure and sodium balance.
Main Types
In general, ACE inhibitors and ARBs have an easily recognizable nomenclature. ACE inhibitors end with the suffix "-pril," and ARBs end with the suffix "-sartan." Renin inhibitors are much newer than ACE inhibitors and ARBs, and aliskiren is the only renin inhibitor currently available in the United States.
Indications for Renin-Angiotensin-Aldosterone System Inhibitors
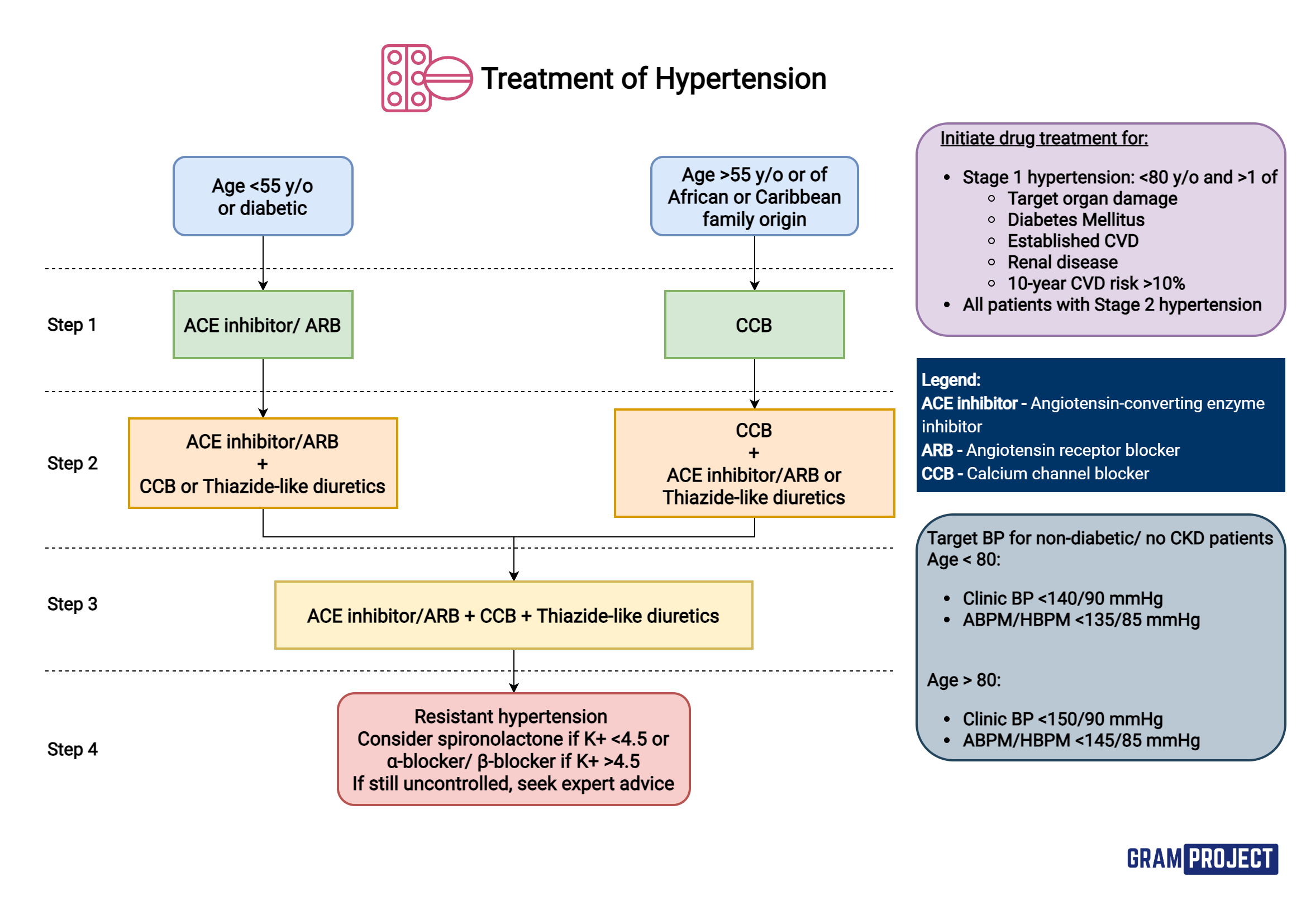
Hypertension
ACE inhibitors and ARBs are first-line medications for treating hypertension, along with thiazide diuretics and calcium-channel blockers. However, if a patient has certain comorbid conditions together with hypertension, ACE inhibitors and ARBs become first-line drugs. For example, if hypertensive patients have congestive heart failure (CHF) or concurrent chronic kidney disease (CKD) with proteinuria (glomerular disease), ACE inhibitors and ARBs are the drug of choice because they slow disease progression.
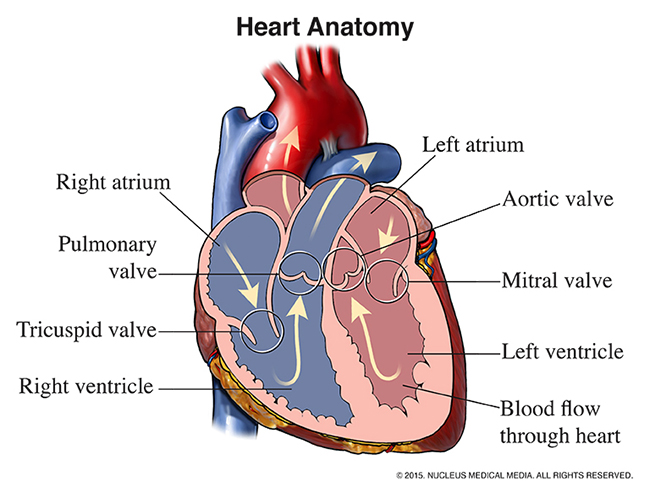
Systolic Heart Failure
Another indication for ACE inhibitors and ARBs is systolic heart failure (also called heart failure with reduced ejection fraction). They improve both symptoms and survival. They are effective in reducing cardiac afterload (pressure against which the ventricle is pumping), which improves cardiac output. Lowering serum aldosterone levels prevents heart failure consequences like ventricular fibrosis and abnormal cardiac remodeling.
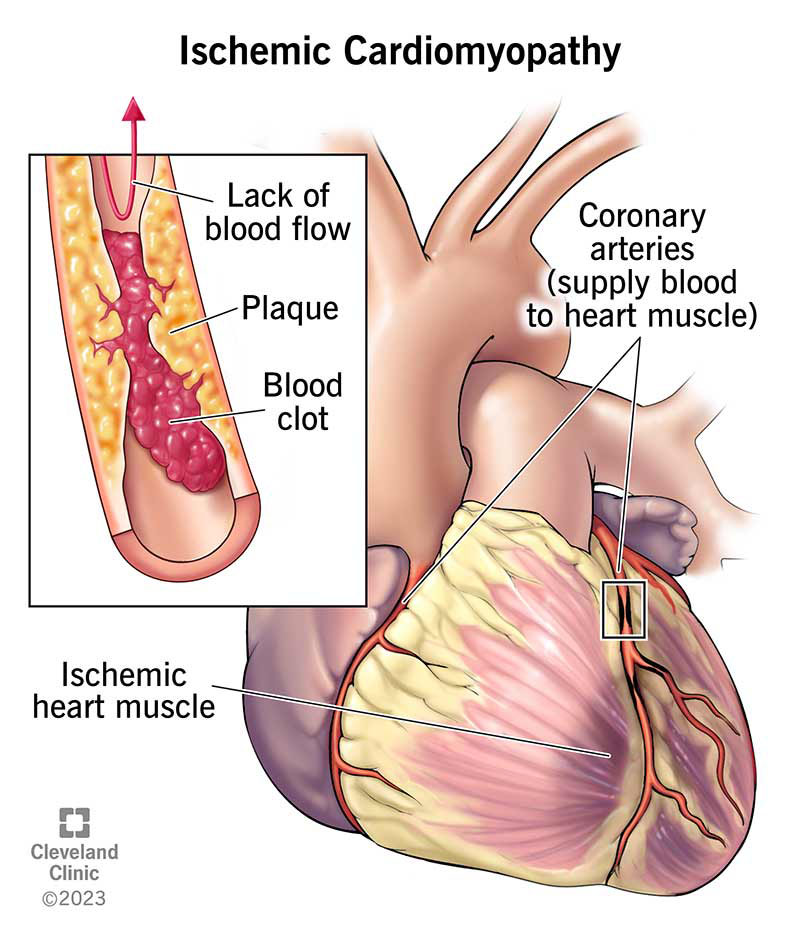
Ischemic Heart Disease
Patients with a history of myocardial infarction (MI) are also treated with ACE inhibitors or ARBs. Treatment reduces morbidity and mortality in these patients, and they are first-line medications on discharge from the hospital, along with aspirin, statins, and beta-blockers.
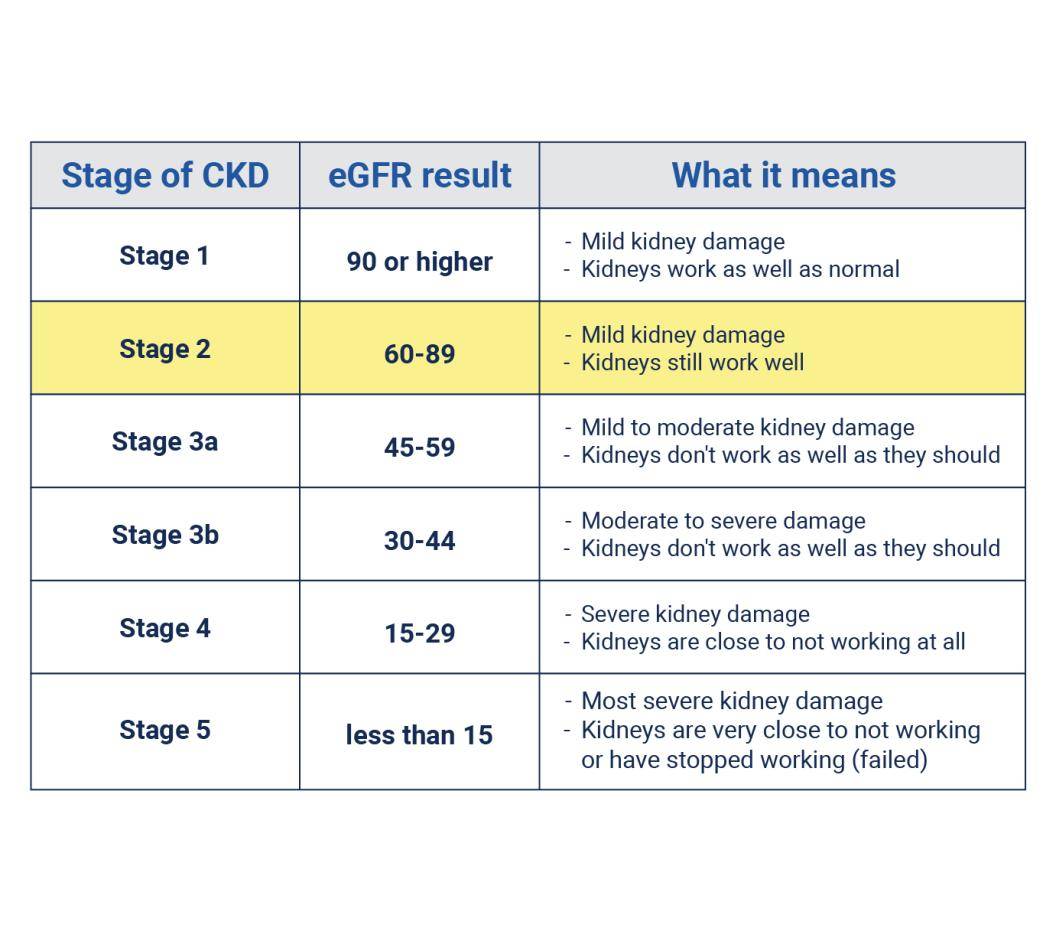
Chronic Kidney Disease
CKD with proteinuria is treated with ACE inhibitors or ARBs to slow disease progression and reduce proteinuria. Among the most important of these chronic renal diseases is diabetic kidney disease, in which early use of ACE inhibitors reduces hydrostatic pressure in the glomerulus and decreases microalbuminuria early in the course, potentially preventing progression of renal disease. Note that CKD without proteinuria does not specifically benefit from use of these drugs, although they may still be used to reduce elevated blood pressure.
Progressive Systemic Sclerosis
Progressive systemic sclerosis is an autoimmune disease of connective tissue that occasionally causes acute kidney injury (AKI) and severe hypertension due to very high renin levels secondary to reduced renal blood flow. ACE inhibitors improve blood pressure, renal function, and survival in these patients.

How Do Renin-Angiotensin-Aldosterone System Inhibitors Work?
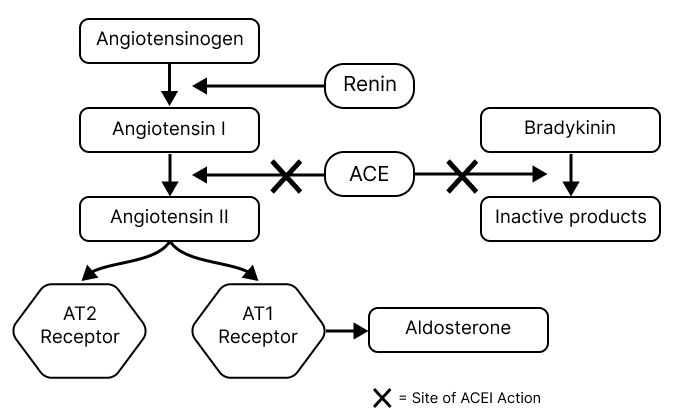
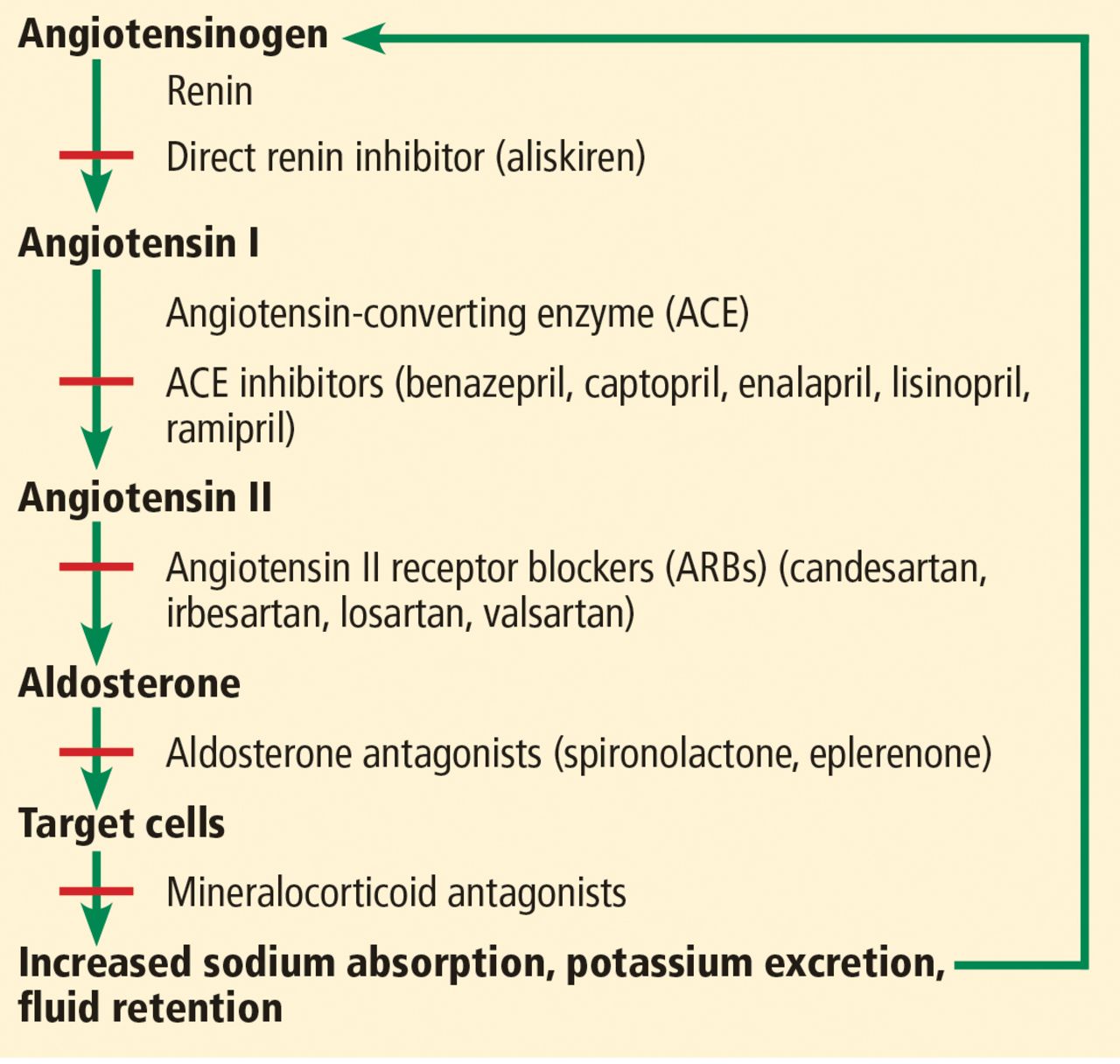
Activation of the RAAS increases both blood pressure and total body sodium (and therefore extracellular and blood volume). ACE inhibitors, ARBs, and renin inhibitors block these effects at various sites along the pathway, making them effective at lowering blood pressure.
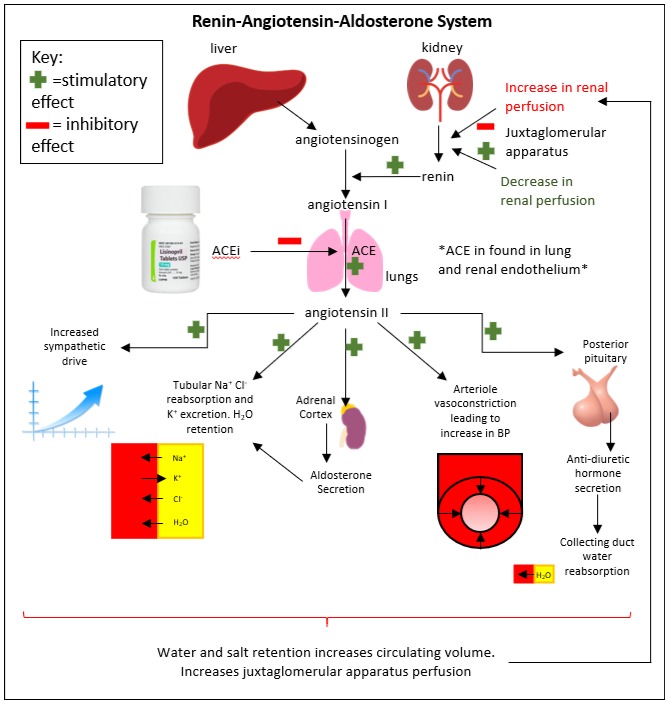
Drug Mechanisms
Renin Inhibitors: Direct renin inhibitors, the newest drug in this group, act at the earliest point in the RAAS. These drugs bind directly to renin and inhibit its binding to angiotensinogen. This reduces the cleavage of angiotensinogen to angiotensin I and subsequently reduces the amount of all other downstream RAAS effectors.
ACE Inhibitors: ACE inhibitors target angiotensin-converting enzyme (ACE), the enzyme that catalyzes the conversion of angiotensin I to angiotensin II. Additionally, ACE plays a large role in the degradation of bradykinin, an inflammatory mediator. The primary expression of ACE in the lungs and subsequent bradykinin accumulation from its inhibition results in some unique side effects of ACE inhibitors.
ARBs: AT-II receptor blockers carry out their effects one step downstream of ACE inhibitors. Instead of inhibiting the formation of AT-II, they block its receptors, limiting its action. The net effect is very similar to ACE inhibitors.