Aortic Aneurysm
Aortic Aneurysm
What Is an Aortic Aneurysm?
An aneurysm is a localized pathologic dilation of a blood vessel. Aneurysms typically arise in arteries and can involve any part of the body. An aortic aneurysm is an enlarged aorta. The aorta is the body’s largest blood vessel and resembles a highway with exits from the left ventricle down to the split at the common iliac arteries. The aorta continuously tolerates high pressure from the heart’s pumping. Given a heart rate of 72 beats/min, the aorta must tolerate 103,680 sharp rises in pressure every day. It’s no wonder the aorta is a common area for aneurysms. The weakened, dilated walls of an aneurysm are prone to rupture, potentially causing catastrophic bleeding.
Types of Aneurysms
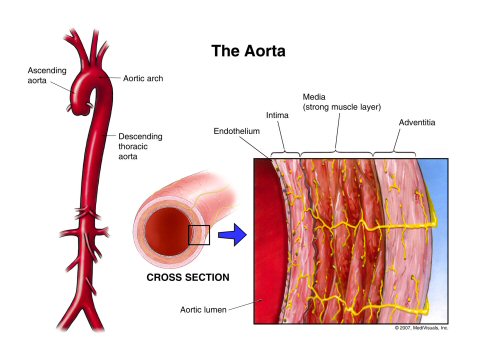
Let’s start by reviewing the general categorization of aneurysms. Recall that vessel walls have three layers:
- Tunica intima: endothelium
- Tunica media: smooth muscle
- Tunica adventitia: protective connective tissue
Depending on the nature of the defect involving these layers, an aneurysm can be categorized as true or false.
True Aneurysm
A true aneurysm is ballooning of the vessel lumen without any defect in the vessel wall; this means that all three layers are involved. True aneurysms can be saccular or fusiform:
- Saccular aneurysms bulge out on only one side of the vessel.
- Fusiform aneurysms bulge out on both sides.
False Aneurysm (Pseudoaneurysm)
A false aneurysm, also known as a pseudoaneurysm, is not dilation of the vessel lumen. Rather, it is a hole that spans all three layers and allows blood to leak out of the lumen into the space immediately outside the vessel. This extravasated blood is contained by extravascular connective tissue, forming a localized hematoma that freely communicates with the vessel.
Thoracic vs Abdominal Aortic Aneurysms
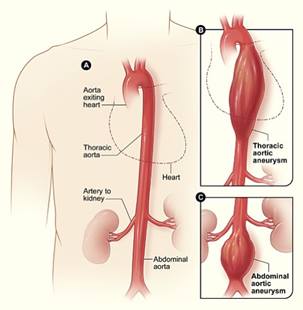
Aortic aneurysms are described based on their location:
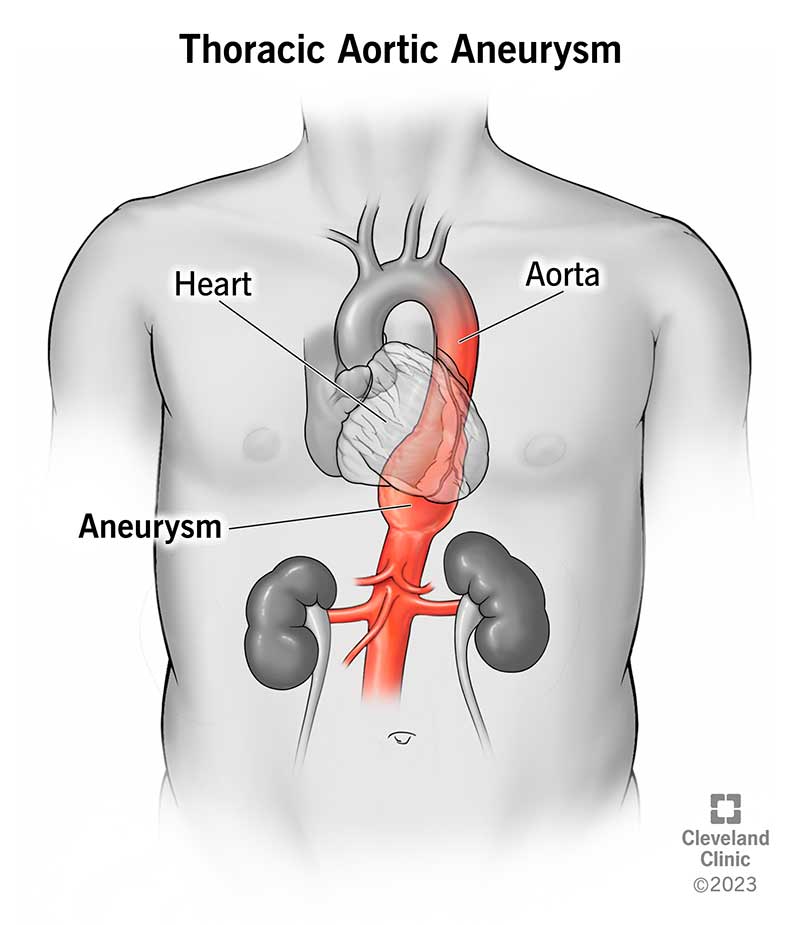
- Thoracic aortic aneurysms (TAAs) involve the aorta within the thorax (ie, above the diaphragm).
- Abdominal aortic aneurysms (AAAs) involve the aorta within the abdomen (ie, below the diaphragm).
Clinical Presentation
An aortic aneurysm is typically asymptomatic until a major, life-threating complication like aortic rupture or dissection occurs. Most aneurysms are discovered incidentally on imaging (eg, CT scan or MRI) done for unrelated reasons or less often found on a routine physical examination as a pulsatile, midline abdominal mass.
If symptoms are present, they are usually nonspecific; chest, abdominal, and back pain are the most common. Less often, patients may present with thromboembolism to the lower extremities from a thrombus originating within the aortic aneurysm, leading to pain in the toes or blue toes.
Thoracic Aortic Aneurysms
Large TAAs can compress intrathoracic structures, leading to:
- Chest pain (compression of coronary arteries)
- Wheezing or hoarseness (compression of the trachea)
- Dysphagia (compression of the esophagus)
TAAs that involve the aortic root (the attachment of the aorta to the heart) may dilate it and pull the aortic valve leaflets apart. This leads to aortic regurgitation, which produces a diastolic murmur that can be heard during chest auscultation and may cause symptoms of heart failure (eg, dyspnea and dizziness).
Abdominal Aortic AneurysmsA patient with a rupturing or dissecting AAA classically presents with sudden onset of severe pain. This can be abdominal pain, back pain, or flank pain. In fact, the sudden-onset, severe flank pain is often confused by clinicians for the pain of kidney stones.
The pain arises because large AAAs can compress intra-abdominal structures such as the branches of the abdominal aorta (eg, inferior mesenteric artery), leading to ischemia. If massive hemorrhage happens, dizziness from the consequent hypotension may result.
