Myocardial Diseases and Cardiomyopathies

Myocardial Diseases
Objectives and Reading
- List and describe the 3 types of cardiomyopathy
- List and describe the common causes of myocarditis
- Describe the types of angina and their underlying causes
- Explain how the distribution of a myocardial infarction can impact patient outcome
- Describe the evolution of a myocardial infarction including post infarct complications
- Read Chapter 10 of Lilly for more information on Cardiomyopathy
- Read Lilly pages 168-171 and 184-189 for more info on ischemic disease

Cardiomyopathies
Cardiomyopathies are a group of diseases that directly involve the myocardium and lead to myocardial dysfunction. They are classified into three main categories:
Dilated Cardiomyopathy
- Description: The most common cardiomyopathy involves progressive cardiac hypertrophy, dilation, and systolic dysfunction. Most cases occur between the ages of 20 to 60.
- Causes: The causes include idiopathic (most common), myocarditis (late stage, most common known cause), genetic factors (e.g., X-linked form involving dystrophin, TTN mutation), and toxic exposures (e.g., alcohol abuse, drugs, organic solvents). Postpartum (peripartum) factors and iron deposition (hemochromatosis or transfusions) can also lead to this condition.
- Morphology (Gross): The heart becomes enlarged and flabby, with a weight that may exceed 900 grams compared to the normal 250-350 grams. There is dilation and hypertrophy of all four chambers, which might be left or right-sided only. Mural thrombi due to stasis may occur, potentially leading to stroke.
- Histology: Features nonspecific changes such as myocyte hypertrophy, interstitial fibrosis (blue), wavy fiber change, and scant mononuclear inflammatory infiltrate.
- Clinical Features: Ineffective contraction, progressive congestive failure refractory to therapy, ejection fraction < 40%, activation of the renin-angiotensin system, arrhythmias, and embolism risks. Prognosis is poor, with idiopathic cases usually fatal, though peripartum cases may spontaneously recover (50%). Cardiac transplantation can be lifesaving.
Hypertrophic Cardiomyopathy
- AKA: Idiopathic hypertrophic subaortic stenosis, Hypertrophic obstructive cardiomyopathy
- Pathogenesis: Most commonly genetic with an autosomal dominant pattern. Key mutations involve genes encoding proteins of the sarcomere such as β-MHC (β-myosin heavy chain) gene (the most common), MYBP-C (myosin-binding protein C) gene, and cardiac troponin T.
- Morphology (Gross): Myocardial hypertrophy predominantly in the left ventricle and interventricular septum, often in the subaortic region causing ventricular outflow obstruction. This can lead to mitral regurgitation and a "banana-like" configuration of the ventricular cavity.
- Clinical Features: Decreased cardiac output, inability to fill the left ventricle, forceful but ineffective ejection, obstruction of left ventricular outflow. Symptoms include dyspnea on exertion, angina, increased pulmonary venous pressure, harsh systolic ejection murmur (increased with Valsalva), ventricular arrhythmias, syncope, atrial fibrillation, risk of infective endocarditis, and myocardial fibrosis. It is a common cause of sudden death in young athletes.
Restrictive Cardiomyopathy
- Description: Characterized by a primary decrease in ventricular compliance, resulting in impaired ventricular filling during diastole. It is the least common type of cardiomyopathy.
- Causes: Can be idiopathic or due to conditions like amyloidosis (primary or neoplastic), myocardial fibrosis (post-surgery), endomyocardial diseases (e.g., endomyocardial fibrosis, Loffler’s syndrome), radiation injury, and storage diseases (iron, glycogen).
- Morphology (Gross): Varies depending on the cause. Common features include atrial dilation ("parachute atria"), endocardial thickening, valvular thickening, and mural thrombi.
- Clinical Features: Stiff and inelastic ventricle that fills with difficulty, similar to hypertrophic subtype. Symptoms include fatigue, exertional dyspnea, chest pain, and signs of systemic congestion (liver, peripheral edema). Outcomes could include systemic emboli, arrhythmias (e.g., AV block), and congestive heart failure.
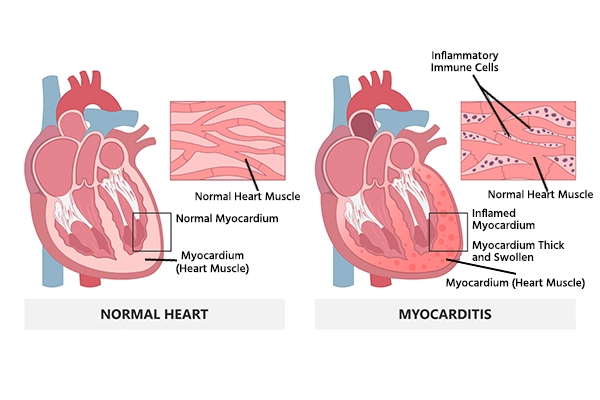
Myocarditis
Myocarditis involves inflammation that leads to injury to cardiac myocytes. Causes include:
- Infectious:
- Viruses (most common in the USA): coxsackieviruses A & B, other enteroviruses, cytomegalovirus, HIV, Parvovirus B19, among others.
- Parasites: Chagas’ disease (Trypanosoma cruzi, most common in South America), toxoplasmosis, trichinosis.
- Idiopathic: Giant cell myocarditis with a horrible prognosis requiring aggressive immunosuppression
- Other Causes: Cardiac allograft rejection, collagen vascular diseases, drug hypersensitivity, sarcoidosis.
Gross Features of Myocarditis:
- Cardiac dilation with hemorrhages
Clinical Features:
Clinical presentation varies from asymptomatic cases to severe congestive failure and arrhythmias. Severe cases may lead to dilated cardiomyopathy.